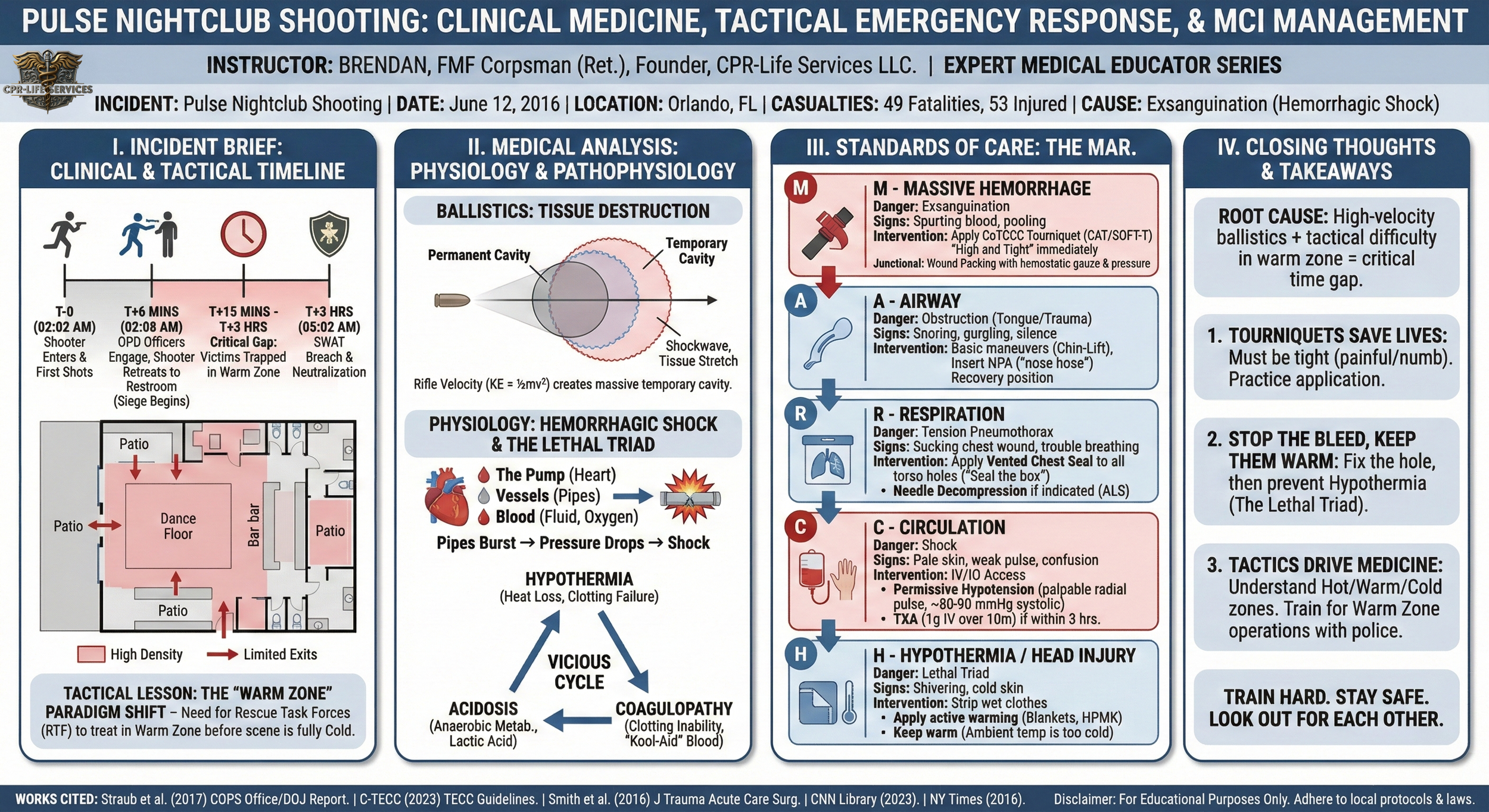
2016 Pulse Nightclub Shooting (Orlando, FL)
· Incident: Pulse Nightclub Shooting
· Topic: Mass Casualty Incident (MCI) Management, Hemorrhage Control, & Tactical Emergency Casualty Care (TECC)
· Date: June 12, 2016
· Location: Orlando, Florida
· Casualties: 49 Fatalities, 53 Injured
· Cause of Death/Injury: Primarily Exsanguination (Hemorrhagic Shock) secondary to Gunshot Wounds (GSW); Penetrating Trauma.
I. Instructor Introduction
Hello. I’m Brendan.
For those of you who don't know me, I spent my early career as an FMF Corpsman with the Marines in Helmand Province, and I’ve spent the years since managing EMS operations and hospital departments. I tell you this not to impress you, but to let you know that what we are discussing today isn't just theory to me. I've seen the chaos of the "hot zone," and I know the weight of the decisions we make there.
Today, we are discussing the Pulse Nightclub shooting. It is heavy. It is tragic. Forty-nine people—sons, daughters, friends—went out for a night of joy and never came home.
We study this loss not to sensationalize it, but to honor them by learning. We study this so that when—not if—the next call comes, your hands are steady, your mind is clear, and your interventions are automatic.
This is a safe space to learn. Ask questions. Challenge the protocols if they don't make sense to you. Let’s get to work.
II. Incident Brief: Clinical & Tactical Timeline
To understand the medical response, you have to understand the tactical reality. Pulse was a nightmare scenario for triage: a loud, dark, confined space with limited exits and a high density of people.
The Environment:
Pulse was a standard nightclub layout—main dance floor, patio, and separate bathrooms. At 2:00 AM, it was "last call," meaning the club was at peak density near the exits and bar areas. The noise level was high (music), and visibility was low (strobe lights, fog). This creates immediate sensory overload for responders and victims.
The "T-Minus" Timeline:
· T-0 (02:02 AM): The first shots are fired near the entrance. The shooter enters the building armed with a Sig Sauer MCX rifle and a Glock 17 handgun. The sound is initially mistaken for part of the music—a common phenomenon in active shooter events called "normalcy bias."
· T+6 mins (02:08 AM): Officers from the Orlando Police Department (OPD) enter the club and engage the shooter, forcing him to retreat into the restrooms. This effectively transitions the event from an "Active Shooter" (dynamic killing) to a "Barricaded Subject with Hostages" (static siege).
· T+15 mins to T+3 Hours: This is the critical gap. While some victims escaped or were dragged out by police during the initial exchange, many wounded remained trapped inside or in the "warm zone" perimeter.
· T+3 Hours (05:02 AM): SWAT breaches the restroom wall with an explosive charge and an armored vehicle (BearCat). The shooter is neutralized at 05:15 AM.
Tactical Lesson: The "Warm Zone" Paradigm Shift
Before Pulse (and incidents like Aurora/Columbine), the old doctrine was "EMS waits until the scene is totally cold." At Pulse, we saw the friction of this. Victims bled out inside while the scene was technically "insecure" but statically contained.
· Takeaway: We must push for Rescue Task Forces (RTF). This is where police protect you (EMS/Fire) so you can enter the "Warm Zone" to stop bleeding before the threat is 100% neutralized. You cannot wait 3 hours to treat arterial bleeding.
III. Medical Analysis: Physiology & Pathophysiology
Let's switch gears to the medicine. The primary mechanism of injury here was multiple high-velocity and handgun ballistic traumas.
Ballistics: The Physics of Tissue Destruction
When a bullet enters the body, it creates two cavities:
1. Permanent Cavity: The hole the bullet physically crushes through tissue.
2. Temporary Cavity: The shockwave that stretches the tissue outward, like a splash when a rock hits water.
With a rifle platform (like the MCX used here), velocity is the key factor (KE = 1/2mv^2). The velocity creates a massive temporary cavity that can tear blood vessels and organs centimeters away from the bullet's path. This is why a rifle wound to the thigh is vastly different from a handgun wound to the thigh.
Physiology: Hemorrhagic Shock
Think of the cardiovascular system like a central heating system in a house.
· The Pump (Heart): Pushes the fluid.
· The Pipes (Vessels): Carry the fluid.
· The Fluid (Blood): Carries the heat (oxygen).
When a patient gets shot, the pipes burst. The system loses pressure.
1. Compensated Shock: The body realizes pressure is dropping. It clamps down the pipes (vasoconstriction) and speeds up the pump (tachycardia). The patient looks pale and anxious, but their Blood Pressure (BP) is normal. Do not be fooled by a normal BP.
2. Decompensated Shock: The body can no longer keep up. The pump is running dry. BP plummets. Mental status fails.
3. Irreversible Shock: Cell death begins. Even if you fix the pipes now, the furnace is broken.
The Lethal Triad
This is what killed many that night. It’s a vicious cycle:
1. Hypothermia: As they lose blood, they lose body heat. Blood clotting enzymes stop working when the body is cold.
2. Acidosis: Without oxygen, cells switch to anaerobic metabolism, producing lactic acid. Acidic blood creates a hostile environment for coagulation.
3. Coagulopathy: The blood loses the ability to clot. It becomes like water ("Kool-Aid").
If you let a trauma patient get cold, they will bleed to death, even if you pack the wound.
IV. Standards of Care: The MARCH Algorithm
In a mass casualty event like Pulse, we don't use standard ABCs. We use MARCH. Why? Because a blocked airway kills you in minutes, but a severed femoral artery kills you in 2 to 3 minutes. Bleeding comes first.
Scenario: You are a paramedic at the triage collection point across the street. A victim is dragged out. They have a GSW to the leg and are unresponsive.
M - Massive Hemorrhage
· The Danger: Exsanguination from extremity wounds (arms/legs) or junctional wounds (groin/armpit).
· Signs/Symptoms: Bright red spurting blood, pooling blood, soaked clothing.
· Intervention:
o Extremity: Apply a CoTCCC-recommended Tourniquet (CAT or SOFT-T) "High and Tight" immediately. Do not check for a pulse first. Just crank it until the bleeding stops. If one doesn't work, apply a second one right below the first.
o Junctional: If the wound is too high for a tourniquet (groin/shoulder), use Wound Packing. Stuff the wound with z-folded hemostatic gauze (like Combat Gauze) right to the bone. Hold pressure for 3 minutes.
o Real World Note: In the dark, you won't see the blood. Sweep the body with your hands. If you feel warm sticky wetness, that is blood. Treat it.
A - Airway
· The Danger: The tongue falling back and blocking the throat due to unconsciousness, or direct trauma to the face/neck.
· Signs/Symptoms: Snoring, gurgling, or silence (silence is bad).
· Intervention:
o Basic: Head-Tilt/Chin-Lift or Jaw Thrust.
o Adjunct: Insert a Nasopharyngeal Airway (NPA)—the "nose hose." It’s fast, easy, and usually tolerated even if they wake up slightly.
o Avoid: Do not intubate (ET tube) in the middle of a firefight or initial triage. It takes too long. Recovery position works wonders.
R - Respiration
· The Danger: Tension Pneumothorax. A hole in the chest lets air into the chest cavity, collapsing the lung and pushing the heart to the side.
· Signs/Symptoms: Sucking chest wound (hissing noise), trouble breathing, unequal chest rise.
· Intervention:
o Apply a Vented Chest Seal (e.g., HyFin or Halo) to any hole from the navel to the neck. "Hole in the box, seal the box."
o If they get worse after sealing, "burp" the seal (lift a corner to let air escape) or perform a Needle Decompression (ALS skill) if indicated.
C - Circulation
· The Danger: Shock.
· Signs/Symptoms: Pale skin, weak radial pulse, confused mental status.
· Intervention:
o IV/IO Access: Establish access but do not flood them with saline.
o Permissive Hypotension: We want a palpable radial pulse (approx. systolic BP of 80-90 mmHg). If you pump their BP up to 120/80 with fluids, you might "pop the clot" and restart the bleeding.
o TXA (Tranexamic Acid): If available and within 3 hours, administer 1g of TXA (slow IV push over 10 mins) to stabilize the clots.
H - Hypothermia / Head Injury
· The Danger: The Lethal Triad (as discussed).
· Signs/Symptoms: Shivering, cold to touch.
· Intervention:
o Strip the wet/bloody clothes.
o Apply active warming (blankets, HPMK kits).
o Myth Buster: "It's Florida in June, they won't get hypothermic." Wrong. A patient in shock cannot regulate body temp. They will cool down to ambient temperature rapidly, and ambient (75°F) is colder than blood (98.6°F). Keep them warm.
V. Closing Thoughts
The Pulse Nightclub shooting highlighted a brutal reality: in a mass shooting, time is the enemy. The gap between the injury and the intervention is where lives are saved or lost. The root cause of the high death toll was a combination of high-velocity ballistics and the tactical difficulty of reaching patients in a "barricaded" warm zone.
Your 3 Takeaways:
1. Tourniquets save lives, but only if they are tight. If the patient isn't screaming in pain (or unconscious), it’s probably not tight enough. Practice putting them on yourself until your fingers go numb.
2. Stop the Bleed, Keep them Warm. If you fix the hole but let them freeze, they die anyway. Hypothermia management starts immediately.
3. Tactics Drive Medicine. You cannot treat a patient if you become a patient. Understand "Scene Safe" isn't a binary yes/no anymore—it's a spectrum (Hot/Warm/Cold). Learn to work in the Warm Zone with police protection.
You all have the capacity to make a difference in chaos. Train hard, stay safe, and look out for each other.
Works Cited
Official Reports:
· Straub, F., et al. (2017). Rescue, Response, and Resilience: A Critical Incident Review of the Orlando Public Safety Response to the Attack on the Pulse Nightclub. Washington, DC: Office of Community Oriented Policing Services. [COPS Office/DOJ].
Clinical Citations:
· Committee for Tactical Emergency Casualty Care (C-TECC). (2023). Tactical Emergency Casualty Care (TECC) Guidelines. C-TECC.org.
· Smith, E. R., Shapiro, G., & Sarani, B. (2016). The profile of wounding in civilian public mass shooting fatalities. Journal of Trauma and Acute Care Surgery, 81(1), 86-92.
News Reports:
· CNN Library. (2023, June 7). Pulse Nightclub Shooting Fast Facts. CNN.
· Alvarez, L., & Pérez-Peña, R. (2016, June 12). Orlando Gunman Attacks Gay Nightclub, Leaving 50 Dead. The New York Times.