TCCC vs. TECC: A Comparative Overview
Hello everyone. It is good to have you here.
As we move into advanced trauma management, a question that almost always comes up is: "What is the actual difference between TCCC and TECC?"
It is a valid question. They look similar, they use similar tourniquets, and they both prioritize stopping the bleed. But as someone who has operated in both a forward-deployed combat environment and as a civilian EMS Operations Manager, I can tell you that the distinction is not just semantic—it is operational.
The mission dictates the medicine. Understanding which guideline applies to your specific operating environment is just as critical as knowing how to pack a wound.
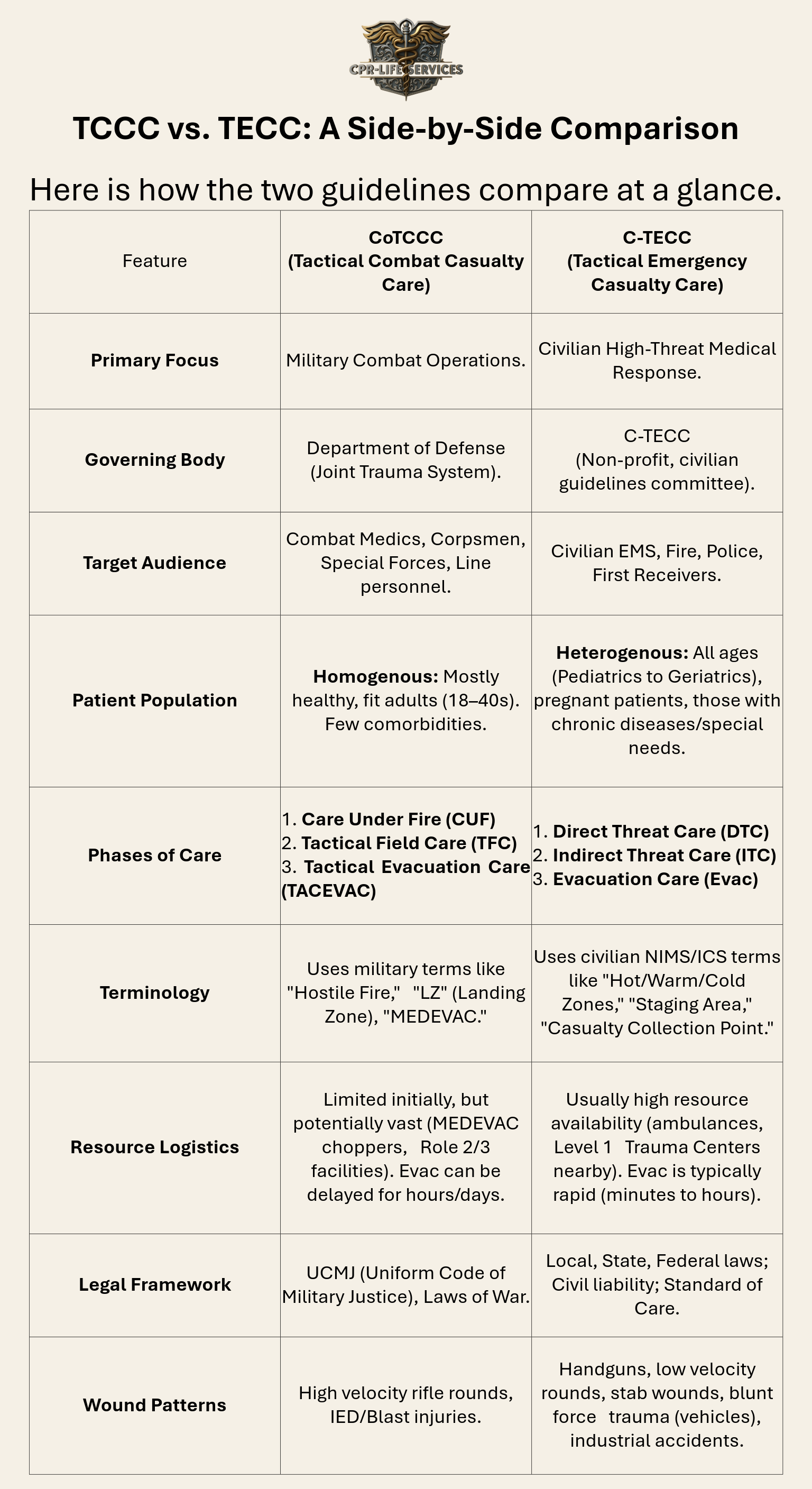
Below, I have broken down the educational rationale for why we study both, followed by a direct comparison to help you visualize where these two protocols align and where they diverge.
Educational Rationale
Why does the distinction matter?
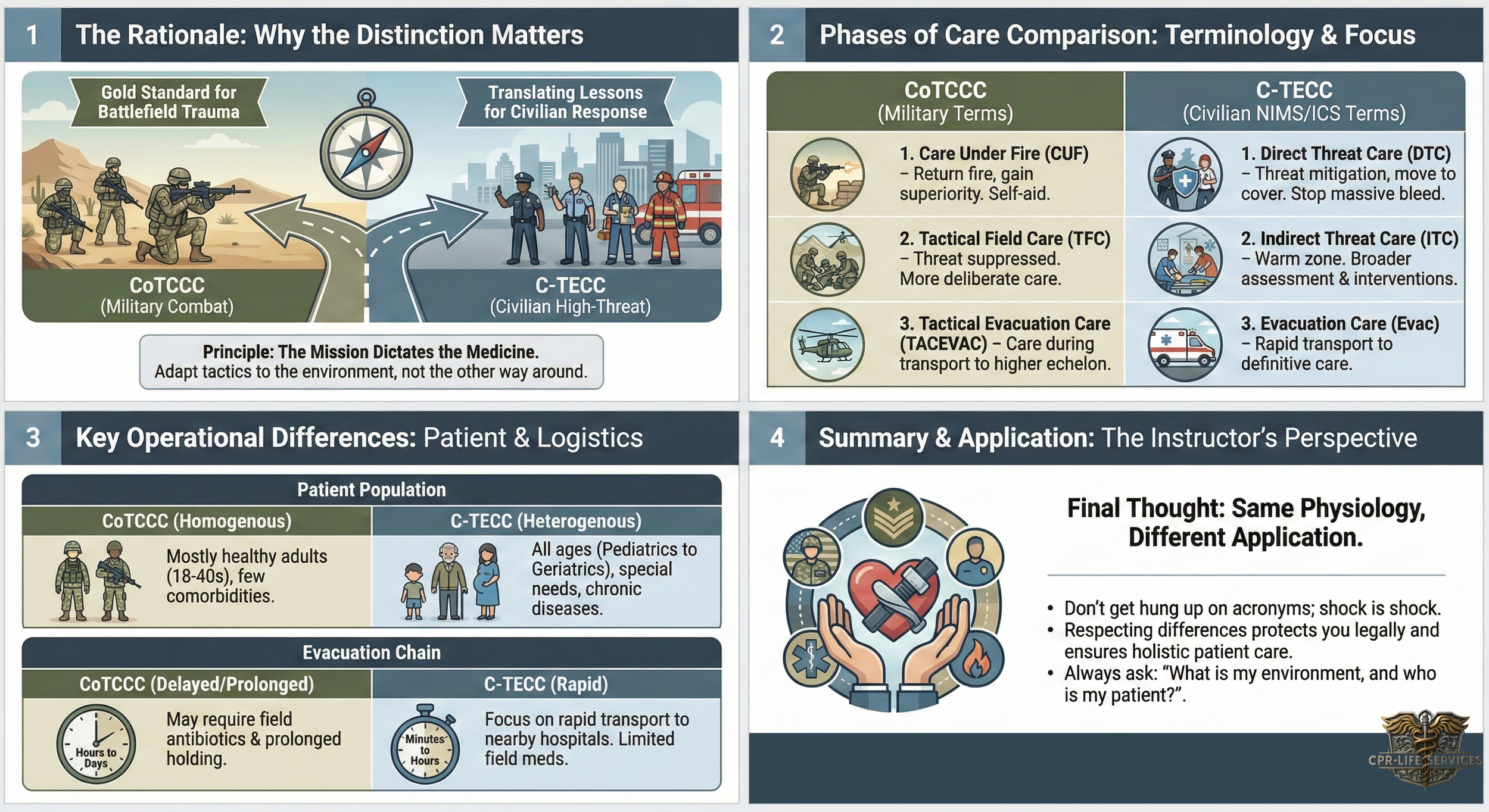
In my time as a US Navy Fleet Marine Force (FMF) Corpsman, the objective was singular: mission accomplishment. The patient population was generally homogenous—young, fit, fighting-age service members. The threat was enemy combatants, and the "rules" were the Laws of Land Warfare.
In the civilian sector, the variables change drastically. As providers, we face different liabilities, a diverse patient population (from infants to geriatrics), and different resource constraints.
We study CoTCCC (Committee on Tactical Combat Casualty Care) because it is the gold standard for trauma care on the battlefield. It is the evidence-based foundation upon which modern trauma medicine is built.
We study C-TECC (Committee on Tactical Emergency Casualty Care) because it translates those battlefield lessons into the civilian high-threat response. It accounts for the grandmother having a heart attack during an active shooter event, or the pediatric patient injured in a blast. It adapts the "tactics" to fit civilian laws and standard operating procedures.
Understanding this difference prevents "tactical rigidity"—it ensures you don't treat a civilian active violence incident exactly like a battlefield in Kandahar, because the logistics and legalities are simply not the same.
Deep Dive: The Three Key Differences
While the interventions (tourniquets, chest seals, needle decompressions) are largely the same, the application differs.
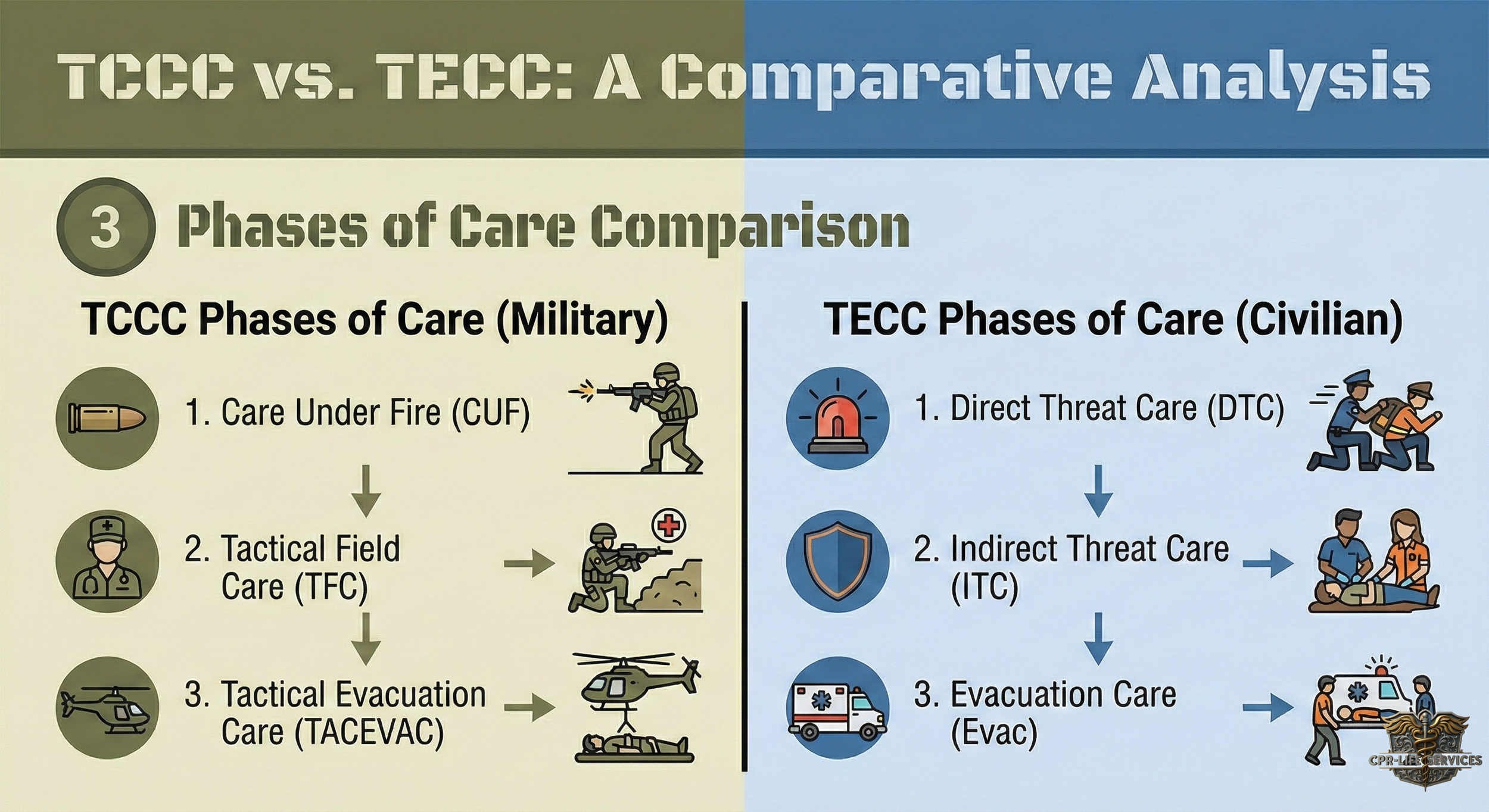
1. The Phases of Care
In TCCC, we use Care Under Fire. This implies you are being shot at by an enemy combatant. Your primary job is to return fire and gain fire superiority.
In TECC, we use Direct Threat Care. In the civilian world, EMS and Fire are rarely armed or expected to "return fire." The priority here is threat mitigation (often by Law Enforcement) and moving to cover. The medical goal remains the same: stop massive hemorrhage if possible, but survival is the priority.
Instructor Note: Notice the shift in language. "Direct Threat" fits better with civilian risk management and OSHA guidelines than "Under Fire."
2. The Patient Population
This is often the most overlooked factor. In the military, I rarely had to worry if my patient was on beta-blockers or blood thinners.
In TECC, you must account for:
Pediatrics: Children have different physiology. They desaturate faster and lose body heat quicker. TECC has specific guidelines for pediatric sizing and drug dosing that TCCC does not prioritize.
Geriatrics: Older adults may not compensate for shock as well as a 20-year-old Marine. Their bones are more brittle; their skin tears more easily.
Comorbidities: A civilian casualty might be diabetic, pregnant, or have a pacemaker. TECC encourages a broader assessment once in the "Indirect Threat" (Warm Zone) phase.
3. The Evacuation Chain
In a combat zone, TACEVAC (Tactical Evacuation) might be a helicopter ride to a Role 2 surgical facility, but it could be delayed by weather or enemy fire for 24 hours. We carry broad-spectrum antibiotics (like Moxifloxacin or Ertapenem) in our combat pill packs because of this delay.
In a civilian TECC scenario, you are usually minutes away from definitive care (a hospital). Therefore, the administration of oral antibiotics or elaborate "field hygiene" is rarely indicated. The focus is on rapid transport to a trauma surgeon.
A Final Thought on Application
Do not get hung up on the acronyms. Whether you call it the "Warm Zone" or "Tactical Field Care," the physiology of shock remains constant. A femoral artery bleed will kill a civilian just as fast as it kills a soldier.
However, respecting the differences protects you legally and ensures you treat the whole patient, not just the wound. When we train together, we will focus on the mechanics of the interventions, but I want you to constantly ask yourself: "What is my environment, and who is my patient?"